The skin disease caused by a fungus on the face is a type of mycosis of smooth skin, but has some features of external manifestations.
Mycosis of the facial skin is caused by a fungus of the genus Trichophyton, so the disease is classified as trichophytosis. The lesion does not involve the area of skin under the beard and mustache in men. The pathology is considered separately from mycosis of smooth skin, since its manifestations are often confused with pityriasis versicolor, rosacea, seborrheic dermatitis, or symptoms of lupus. Therefore, treatment for mycosis of the facial skin is prescribed by a dermatologist only after a thorough diagnosis.
The disease is quite rare. Infection occurs mainly through transmission of the pathogen:
- from animals;
- less often from a sick person to a healthy one.
At the same time, foci of infection may appear on the scalp or torso.
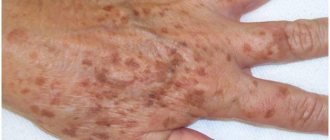
Mycosis of the facial skin causes not only health problems. Its signs are clearly visible and therefore cause aesthetic discomfort in the patient and surrounding people.
Signs of the disease are presented in the photo of facial skin mycosis:
General information
Fungal diseases are infectious diseases caused by pathogenic and opportunistic fungi.
Currently, the number of fungal infections is growing, which is associated with the expansion of risk groups and climate change. Risk groups include people with allergic conditions, malignant neoplasms, those who have undergone organ and stem cell transplants, patients with immunological diseases, those who have undergone complex operations and who have received massive antibacterial therapy. Superficial skin lesions can be caused by dermatophytes, molds and yeast-like fungi. Dermatophytes rank first in the list of causative agents of skin diseases, and they are grouped into three large genera: Trichophyton, Microsporum and Epidermophyton. Mycosis on the skin of the face (Tinea faciei) is considered a variant of mycosis of smooth skin, but is less common than mycoses of other localizations.
Most often, facial damage is caused by T. rubrum (rubromycosis disease) and T. mentagrophytes, less commonly by microsporum fungi: M. Canis and M. audouinii. Dermatophytosis of the face can be detected as an independent primary lesion, or be secondary in nature when the process spreads from primary lesions to the trunk, folds, neck or limbs. This is facilitated by concomitant pathology of internal organs, diabetes mellitus , pathology of the thyroid gland, as well as the lack of treatment for mycotic lesions. Facial mycosis caused by dermatophytes occupies a separate place in the classification - ICD-10 code B35.0. The most common yeasts that affect the skin of the face and scalp are Candida and Pityrosporum ovale yeast.
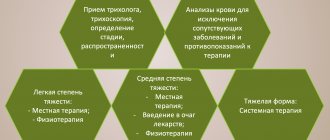
Diagnosis of fungal infection
To diagnose a fungus in the body, it is necessary to identify the clinical signs characteristic of a given disease, and then conduct a series of laboratory tests to identify the type of fungal infection (this is extremely important for further treatment).
Laboratory tests necessary to diagnose a fungal infection:
- Aspergillus fumigatus, DNA [PCR];
- Candida albicans, IgG, titer and DNA [real-time PCR];
- Analysis of vaginal microbiocenosis, including 8 indicators and quantitative DNA [real-time PCR];
- Sowing Candida spp, yeast-like fungi.
Other tests needed to diagnose a fungal infection:
- Ultrasound, which allows you to identify space-occupying formations of a pathological nature that may occur due to a fungal infection affecting internal organs.
Pathogenesis
The main location of pathogenic fungi is keratin-containing tissues (the stratum corneum of the epidermis, nails and hair), since they feed on keratin and actively multiply in these tissues. Dermatophytes penetrate the keratin of the skin using keratinolytic proteases. They also produce multiple proteases that destroy other proteins - fibrin , collagen , elastin .
The introduction of a fungus into the skin does not always cause the development of an infectious process. Thus, in the absence of skin damage, long-term asymptomatic carriage of pathogenic fungi occurs. For the development of the disease, certain conditions are necessary: viability, the number of fungi on the skin, the body’s ability to resist pathogens. Mycotic infection is resisted by the barrier function of the skin and immune . Patients with weakened immune systems are susceptible to fungal infections. Elimination of pathogens depends on the condition and function of phagocytic cells - macrophages and neutrophils. The former provide antifungal protection at the initial stages of infection, and neutrophils eliminate fungal invasion.
Having penetrated the skin, the fungus forms threads of mycelium, which penetrate into healthy areas of the skin, causing characteristic damage. If the rate of exfoliation of the stratum corneum (desquamation) is low, then the rate of growth of the fungus prevails and the infectious process spreads quickly. If the rate of desquamation exceeds that of the fungus, then the infection does not spread, since the fungus is eliminated with dead scales of the stratum corneum.
Who is at risk for fungal infection?
- People who sweat intensely;
- People whose immune systems are weakened (say, if a person is taking glucocorticoid drugs);
- Patients suffering from diabetes;
- People who work in warm and humid conditions;
- People walking barefoot in public places (swimming pools and gyms);
- People who wear poorly ventilated clothing, shoes, socks;
- People who neglect the rules of personal hygiene, use other people's towels and bed linen, wear someone else's shoes;
- Patients who have completed a course of antibacterial therapy;
- People who are in areas where the prevalence and incidence of one of the types of fungal infections is endemic.
Classification
In the classification of all mycoses, the following lesions are distinguished:
- Superficial ( dermatomycosis ).
- Deep subcutaneous lesions.
- Visceral mycoses (damage to internal organs).
Superficial mycoses are classified according to the localization of the process:
- Mycosis of the feet.
- Smooth skin of the body.
- Inguinal mycosis.
- The scalp.
- Mycosis of the hands.
- Onychomycosis (damage to nails).
- Mycosis of the face.
Facial dermatophytosis is most often found in countries with warm climates. There are two forms: classic and with deep inflammatory lesions. In the first form, the lesion is represented by flat scaly papules, the borders of which are raised and enlarged, turning into a ring-shaped lesion. The desquamation border contains elevated papules and vesicles. The merged elements occupy large areas.
Deep lesions are caused by the fungus Trichophyton verrucosum, which is transmitted from cattle. Large inflammatory foci with a raised surface and pustules appear on the skin of the face. A secondary bacterial (staphylococcal) infection is often associated. The process resolves with hyperpigmentation and scarring .
Features of facial skin infections
The blood supply to the organs of the head, face, and membranes of the brain is closely connected. Incorrect treatment and squeezing of pimples is dangerous due to the spread of bacteria through the blood and lymph. You can achieve an increase in the area of the affected area, such dangerous complications as meningitis, abscesses and phlegmon, and inflammation of the eyes.
Before deciding on cosmetic procedures - cleansing, peeling, mesotherapy - undergo an examination by a dermatologist to determine the cause of the pustular rash and receive treatment.
Causes
Fungal infection occurs:
- Zoophilic fungi Microsporum and Trichophyton in direct contact with animals (cats, dogs, cattle). Animals of any breed are susceptible to infection. Most often, the lesion is caused by Trichophyton, rarely by M. canis. Microsporum canis is spread by cats. Trichophytosis is common among horses, mice, rats, and pigs. There are cases of Trichophyton Arthroderma infection from guinea pigs. Trichophytes infect any area of the skin causing acute infections.
- Through infected objects, instruments and skin flakes.
- With autoinoculation - transfer of the pathogen from other foci of dermatophytosis (torso, limbs, scalp).
Most often, microsporia occurs in children. Infection occurs in the summer during contact with sick cats, and appears in the autumn when returning from vacation. Facial dermatophytosis is very common in athletes (wrestlers) and is caused by Trichophyton tonurans. Dermatophytosis of the beard area is caused by the fungi Trichophyton mentagrophytes, Trichophyton rubrum, and rarely Microsporum canis.
Symptoms
You can think about a fungal infection of the skin of the face if you have any rash with scales. Signs of inflammation may be absent or mild in dermatophyte infections caused by Trichophyton rubrum. Clinically, mycosis of the face can manifest itself as typical round pink spots surrounded by an edematous ridge of vesicles and pustules. These spots increase along the periphery, and their central part is covered with scales (this form is called circinar).
The lesions are most often localized in the area of the lower lip and chin. Hair in the lesion rarely becomes infected. In atypical forms, edematous erythema appears with or without peeling, which is accompanied by itching and burning. It is also possible to develop an infiltrative-suppurative form with the appearance of bluish-red nodes with a bumpy surface. Merging, numerous pustules form abscesses. In this case, the hair in the lesion is affected and can be easily removed without pain.
Microsporia
It appears as erythematous plaques with clear boundaries, which are often covered with gray-white scales. Increasing in size, the plaque takes on a ring-shaped shape, resolves in the center and has a raised red ridge along the periphery. Sizes range from 1 to 8 cm in diameter.
Photo of fungus on the face (microsporia)
Most often, plaques are located asymmetrically. They are localized on the cheeks and chin, less often on the forehead, nose and near the eyes. The patient may complain of itching, and there is also increased sensitivity to sunlight. Microsporia of the face is similar in appearance to the rash of lupus erythematosus , eosinophilic granuloma of the face and lymphocytic infiltration.
Rubrophytia
Caused by the fungus Trichophyton rubrum. Lesions of smooth skin with it have any localization, including the face, which is less common than lesions of large folds, buttocks and legs. In typical cases, rubromycosis appears as pink or bluish spots that have rounded outlines and are clearly demarcated from unaffected skin. Small scales are visible on the surface of the spots, and a ridge of papules, vesicles and crusts forms along the periphery.
The spots are small, but increase in size due to peripheral growth. Over time, the inflammation subsides, the blisters disappear, and the peripheral ridge becomes flat. The spots become bluish and brownish in color.
Fungus on eyelids
Fungal blepharitis is a fungal infection of the skin of the eyelids, caused by the spread of the pathogen from neighboring lesions on the face. Most often these are yeast fungi Malassezia furfur and Candida. Deficiency of T-cell immunity predisposes to the development of infection with yeast-like fungi. It is most likely that Candida fungi are transferred from other areas to the eyelids by hand. There are also cases of fungal blepharitis after corneal transplantation. In this case, it may be due to long-term use of corticosteroids.
Characteristic symptoms are swelling of the eyelids, the skin of the eyelids is covered with scales, under which there may be erosion. The process often extends beyond the skin of the eyelids to the area around the eyes.
Candidiasis
Isolated candidiasis of the lips spreads to surrounding tissues - the corners of the mouth and the skin of the face. Candidal angular cheilitis occurs when oral candidiasis and infection of the corners of the mouth. This is facilitated by saliva flowing into the corners of the mouth.
This pathology affects both corners of the mouth. The disease begins with redness and itching. Then cracks form in the area of the corners, painful when opening the mouth, touching and moving the lips. Erosion forms on the cracks, along the edge of which the epidermis peels off. With candidiasis, erosions have a whitish coating. This process enters the chronic stage.
Any localization of skin candidiasis begins with persistent itching. A main focus of bluish-red color with a moist, shiny surface appears, and screenings appear in the form of small superficial blisters and pustules. Surface erosions and cracks form at the source. The surface of the erosions is red, bordered by a white rim.
Fungus in the nose
Also common are ENT mycoses, the causative agents of which are opportunistic fungi (Candida and Aspergillus). These conditions occur when immunity . There are not only fungal pharyngitis and otomycosis (ear damage), but also mycoses of the nose (occur in 14% of cases) and paranasal sinuses. In more than half of patients suffering from chronic sinusitis , it is caused by fungi. In this case, the mycelium grows inside the sinus cavity and does not grow into its mucosa. The disease develops slowly - from the moment the inflammation begins until the initial symptoms appear, it takes from two to 15 years.
Symptoms of a fungus in the nose include constant nasal congestion and heavy discharge, which depend on the stage of the process. Signs of fungus in the nose also include severe soreness of the nasal mucosa. For fungal infections of the nose and sinuses, systemic therapy is prescribed - Intraconazole 100 mg per day or Medoflucon 50 mg per day are taken orally. The effectiveness of both drugs is 93%.
Publications in the media
Fungal infections of the skin and its appendages have been known since ancient times. Doctors gave skin diseases with different symptoms from others separate designations (for example, favus), not yet knowing that they were caused by fungi. The history of the science of dermatophytes began with the discovery of the favus pathogen Achorion schoenleinii in 1839 by Schonlein JL. Schonlein found fungal mycelium in the skin rashes of a patient whom he had mistakenly diagnosed as having impetigo. In 1841, Grubi D. established the relationship between skin diseases and fungi. He described the clinical picture of microsporia and the morphological features of the fungus that causes this disease. As a result of the use of the special nutrient medium proposed by Sabouraud R. for the cultivation of mushrooms, favorable conditions were created for mycological researchers. Relevant clinical and laboratory studies began to be carried out, and the era of discovery of new types of pathogens began. In the field of medical mycology, significant changes have occurred in various directions: dermatophytes, molds, yeast-like fungi, the pathogenesis of mycotic infections were studied and described in detail, the nature of actinomycosis was determined, the treatment of fungal diseases was improved, etc. Russian scientists also made a significant contribution to the development of medical mycology , among whom the most famous are P. N. Kashkin, A. M. Arievich, N. D. Sheklakov, O. K. Khmelnitsky, A. N. Arabian, Z. G. Stepanishcheva, N. A. Krasilnikov, G. O Suteev, V. M. Leshchenko and many others.
Fungal diseases have long gone beyond the specialty of a dermatologist, but dermatologists-mycologists are still doing a lot of work to combat dermatomycosis, which ranks first in prevalence in all countries.
Superficial mycoses (dermatomycosis) include infections that affect the skin, nails and hair. The main pathogens are dermatophytes, fungi that can absorb keratin. These include fungi of the genera Microsporum, Trichophyton and Epidermophyton, which, depending on the source of infection, are divided into anthropophilic, zoophilic and geophilic. The habitat of zoophilic dermatophytes (Trichophyton mentagrophytes v. gypseum, T. verrucosum, Microsporum canis, etc.) is animals, anthropophilic (Trichophyton rubrum, T. mentagrophytes v. interdigitale, Microsporum ferrugineum, Epidermophyton floccosum, etc.) is human, geophilic species ( Microsporum gypseum) live in the soil. Dermatophytes are highly contagious and can be transmitted to humans from humans, animals or soil, causing disease. The main “spreaders” of infection are anthropophilic species.
Superficial mycoses also include keratomycosis: pityriasis versicolor and piedra, which affect the most superficial areas of the stratum corneum and hair cuticle. The causative agent of pityriasis versicolor and seborrheic dermatitis, the yeast-like fungus Malassezia furfur, lives on the skin of humans and animals and, under favorable conditions, can affect the stratum corneum of the epidermis and the mouth of the follicles. The disease in most cases is not contagious. White and black piedra are usually found in countries with hot and humid climates. The diseases are less contagious. The causative agent of black piedra, Piedraia hortae, is found only on hair. Trichosporon beigelii is widespread in the environment and, in addition to white piedra, can also cause skin and nail lesions.
In addition to true dermatophytes, which infect only the skin and its appendages, superficial mycoses can also be caused by other fungi, isolated from a variety of localizations during systemic mycoses. Candida spp. - the second most common discharge in dermatomycosis and onychomycosis after dermatophytes. Up to 40% of cases of onychomycosis of the hands are caused by Candida. Lesions of yeast-like fungi on the scalp with a clinical picture of seborrheic eczema were noted. Superficial forms of candidiasis also include lesions of the mucous membranes of the oral cavity and genital organs.
In cases of onychomycosis caused by molds, there is still doubt about the ability of these opportunistic pathogens to independently infect nails due to their weak proteinase and keratinase activity. It is known that mold fungi can manifest themselves as a secondary infection, penetrating into tissues already affected by dermatophytes. However, as a result of many years of research, it has been proven that some molds can penetrate into the intercellular nail space using perforating organs. The most common causative agents of mold lesions of the skin and nails are Scopulariopsis brevicaulis, Pyrenochaeta unguis-hominis, Aspergillus spp., Fusarium spp., Alternaria spp., Cladosporium spp. and etc.
There are numerous options for the classification of fungal infections, which to a greater or lesser extent take into account the etiology, pathogenesis, clinical picture and features of the epidemiology of diseases. In domestic dermatology, the classification of N. D. Sheklakov is most often used:
- Keratomycosis (lichen versicolor, piedra, imbricated mycosis).
- Dermatophytosis (athlete's foot, trichophytosis, microsporia, rubromycosis, favus, etc.).
- Candidiasis (superficial candidiasis of the skin and mucous membranes, visceral, etc.).
- Deep mycoses (chromomycosis, sporotrichosis, etc.).
- Pseudomycosis (erythrasma, actinomycosis, nocardiosis, etc.).
However, many countries around the world have adopted a classification of fungal diseases according to the localization of the pathological process:
- Tinea pedis - mycosis of the feet.
- Tinea corporis is a mycosis of the smooth skin of the trunk.
- Tinea cruris - inguinal mycosis.
- Tinea capitis is mycosis of the scalp.
- Tinea unguim - onychomycosis.
- Tinea manum - mycosis of the hands.
- Tinea barbae is mycosis of the face.
This classification is convenient from a practical point of view, but does not take into account the etiological features of dermatophytosis, which can determine the nature of epidemiological measures and treatment features.
Main clinical features of fungal infections
Mycoses of the feet (Fig. 1). The interdigital folds and soles are mainly affected. In the interdigital folds, slight peeling with minor inflammatory phenomena, moderate maceration, cracks, and blisters are observed. On the sole there is thickening of the stratum corneum, flour-like peeling in the skin grooves, small cracks on a slightly hyperemic background. In the dyshidrotic form, numerous blisters form on the skin of the arch and inferolateral surface of the foot, which then merge to form large blisters. In place of the opened blisters, erosions with an uneven edge remain.
Mycosis of smooth skin of the body (Fig. 2). With tinea versicolor, brownish and white spots are usually localized on the skin of the chest, back, neck and shoulders. Scaly lesions have clear boundaries and are not accompanied by inflammatory phenomena.
When the skin is damaged by other pathogenic fungi, clearly demarcated, round, swollen lesions with a raised ridge are formed. The center of the lesion is flattened, with slight peeling. The lesions increase due to peripheral growth.
Mycosis inguinal. Typical localization is the inner thigh, lower abdomen, buttocks. The lesions are clearly defined, scaly, erythematous, with an inflammatory ridge. Over time, the general moderately erythematous background gives way to a brownish one.
Mycosis of the scalp. Most often observed in children. The disease manifests itself as large, round, clearly demarcated, scaly patches of baldness. Inflammatory phenomena are mild. Discolored hair within the lesion is broken off a few millimeters above the skin level (with microsporia) or, breaking off at the skin level, leaves a stump in the form of a black dot (with trichophytosis). Zoophilic pathogens can cause the development of an infiltrative-suppurative form of dermatophytosis: the lesion protrudes above the surrounding skin, is covered with purulent-bloody crusts, and hair falls out.
Onychomycosis. Various types of fungal infection of the nail plates are characterized by loss of transparency, discoloration (whitish, yellowish), thickening, subungual hyperkeratosis, crumbling or destruction down to the nail fold.
Mycosis of the hands. In the squamous form of palm lesions, the disease manifests itself in fine-lamellar mealy peeling in the skin grooves. Cracks may form, accompanied by pain and itching. In the dyshidrotic form, vesicles form, which often cluster and can coalesce to form blisters.
Mycosis of the face. Most often, lesions are localized in the neck, chin and lower lip. The infiltrative-suppurative form of the lesion manifests itself in the formation of large bluish-red nodes with a bumpy surface. Numerous pustules merge to form abscesses. Changed dull hair in the lesion is removed easily and without pain. The superficial version resembles mycosis of smooth skin.
Laboratory diagnostics
Microscopy of clinical material is a quick and simple method for preliminary diagnosis of the disease. In cases where there is no growth of the pathogen in culture, a positive result of direct microscopy can be an undoubted confirmation of a mycotic infection. In scrapings from skin and nails, dermatophytes are usually represented by thin, 2–4 µm in diameter, straight and rarely branched mycelium. Often in the preparation one can find atypical forms of dermatophyte mycelium - chains of round arthrospores (Fig. 3).
M. furfur, when microscopy of skin scales, is revealed in the form of round cells with a diameter of 3–8 μm, collected in clusters, and short curved mycelial hyphae of a characteristic “banana-shaped” shape. In most cases, the diagnosis of lichen versicolor can be established precisely by microscopy of the native specimen, since culture of the material usually does not give results.
Scopulariopsis brevicaulis in nail scales is represented by characteristic cup-shaped spores with a rough shell.
Fungi of the genus Candida form typical budding yeast cells and pseudomycelia (branching chains of long cells).
Identification of other pathogens in native preparations is difficult.
When hair is damaged by dermatophytes, several tissue forms of the fungus are observed: 1) endoectothrix - spores with a diameter of 2–3 microns are “mosaic” located inside and mostly outside the hair, forming a muff on the root (“Adamson’s sheath”). Inside the hair you can also see mycelium, which, with light pressure on the preparation, comes out of the hair in the form of a fringe - “Adamson's brush”. The causative agent is Microsporum spp.; 2) endothrix - spores with a diameter of 4–6 microns are located inside the hair in longitudinal chains, completely filling it. The causative agent is Trichophyton spp. The final identification of fungi is carried out by cultural studies.
For cultural studies of pathological material, Sabouraud's medium with chloramphenicol and gentamicin is used, as well as for the selective isolation of dermatophytes - with cycloheximide (actidione), to inhibit the growth of fast-growing saprophytic fungi.
Dermatophyte genera are distinguished by the presence and morphology of multicellular macroconidia and unicellular microconidia.
Characteristics of the most important pathogenic fungi
Epidermophyton floccosum. Anthropophil. Affects the skin of the groin folds and legs. Colonies grow slowly, grayish-brown, lemon-olive, later white, folded-lumpy in the center. The surface of the colony is leathery or velvety-mealy. By microscopy: in mature cultures there are chains of intercalary chlamydospores. Macroconidia are 4–5-celled, club-shaped, smooth, with rounded ends. Arranged in bunches of 3–5 pieces. Microconidia are absent.
Microsporum canis (Fig. 4). Zooanthropophil. The most common pathogen of microsporia in Russia. Colonies are fast-growing, flat, radiant-hairy. The mycelium is grayish-white, against the background of a brownish-red or orange reverse side, the general hue of the colony is salmon. Under microscopy: it forms a characteristic bamboo-like mycelium, there are combs, short spirals, intercalary chlamydospores. Macroconidia are fusiform, pointed, spinous, multi-chambered (4–12 cells) with a distinct double-circuited shell. Microconidia are pear-shaped and occur inconsistently.
M. gypseum. Geophilic pathogen. It affects the skin and hair primarily of people who cultivate the soil. The colonies are fast-growing, flat, mealy (powdery), later with a small velvety elevation in the center. The color is yellowish-pink. The reverse side is yellow. Under microscopy: numerous macroconidia (4–6 cells) spindle-shaped, wide, blunt-ended, smooth. Microconidia, if present, are numerous and pear-shaped or oval.
Trichophyton rubrum (Fig. 5). Anthropophil. The most common causative agent of dermatomycosis. Affects toenails, hands and skin anywhere on the body.
The colonies are velvety, white, sometimes waxy at the beginning of growth; later they can acquire a pinkish or purple-red color. The reverse side is yellow, red or cherry red. Under microscopy: abundant microconidia of elongated, drop-shaped or pear-shaped are located on the sides of the mycelium. Macroconidia are 5–6-celled, blunt-pointed.
T. mentagrophytes var. interdigitale. Anthropophil. Affects the nail plates and skin of the feet.
Colonies are fast-growing, velvety, white, sometimes pinkish. With age, the colonies of different strains become fluffy or densely powdery. The reverse side is colorless or brownish. Under microscopy: microconidia are round, located on the sides of the mycelium, singly and in clusters. Cigar-shaped, 3–5-celled macroconidia with a rounded end are rare. In mature cultures there are many whorls and spirals, nodular organs and intercalary chlamydospores are formed.
T. mentagrophytes var. gypseum. Zooanthropophil. Affects skin and hair. In terms of frequency of isolation, it ranks second after T. rubrum.
Colonies are fast-growing, flat, granular-powdery, white, cream, yellowish. The reverse side is brownish-red. Under microscopy: microconidia are abundant, round, located on the sides of the mycelium singly and in the form of clusters. Macroconidia are cigar-shaped, 3–8 cells with rounded ends.
Treatment
Therapy for various mycotic lesions of the skin and nails is carried out with antifungal drugs, which can be systemic or applied externally. In practice, both monotherapy and various combinations of antifungal drugs are used. In most cases, treatment should be comprehensive using external antifungal agents, systemic drugs, and symptomatic treatment. Methods and means of topical therapy are mandatory components of the treatment of various mycotic skin lesions. If the fungal process is in the initial stage and there are minor skin lesions, then it can be cured by prescribing only external antifungal drugs. With a widespread or deep mycotic process, as well as in patients with damage to hair and nails, treatment may be difficult.
Antifungal drugs or antimycotics are specific agents used to treat fungal infections of the skin, nails, hair, etc. They may have fungicidal and fungistatic properties. The fungicidal effect of the antifungal agent leads to the death of fungal cells, while the fungistatic effect stops the formation of new fungal cells. Antimycotics are conventionally divided into 5 groups: polyene antibiotics, azole compounds, allylamine drugs, morpholine derivatives and medications without a clear relationship to any specific group.
When prescribing topical therapy, it is important to take into account the nature of the specific effect of the antifungal agent. It is known that griseofulvin preparations are active only against dermatophytes. External products containing polyene antibiotics - against yeast and mold fungi, preparations of selenium, zinc, benzyl benzoate - fungi of the genus Malassezia and the causative agent of erythrasma Corynebacterium minnutissium. Modern antifungal agents of the azole, allylamine, morpholine series, thiocarbamycins and pyridine compounds have a significantly wider spectrum of antifungal activity, as well as anti-inflammatory and antipruritic properties and are well tolerated.
Onychomycosis is the most treatment-resistant disease. The basis for success is an individually selected treatment regimen. When treating, it is necessary to take into account the patient’s age, concomitant diseases, the number of affected nails, and the degree of involvement of the nail plates in the pathological process.
Currently, mycologists have a large arsenal of agents with a wide spectrum of fungicidal action, accumulation in therapeutic concentrations in the nail plate and nail bed. The greatest preference is given to drugs that meet the requirements for therapeutic effectiveness, as well as aesthetics and ease of use.
Treatment of onychomycosis is divided into local, systemic, and combined.
Local treatment allows you to create high concentrations of the drug on the surface of the nail plate. However, the active ingredients of the antimycotic do not always penetrate into the nail bed, where the most viable fungi are located, in effective concentrations.
Local antimycotics: varnishes - Loceryl, Batrafen; creams - Lamisil, Nizoral, Mikospor, Mifungar, Travogen, Ecozax, Exoderil, Pimafucin, sprays - Daktarin, Lamisil, etc. It is necessary to take into account that they are not intended specifically for the treatment of onychomycosis, but they can be used in the treatment of fungal infections of the skin of the feet, interdigital gaps, often combined with onychomycosis.
To treat nails, local antiseptics are also used - alcohol solutions of iodine and dyes.
Multicomponent preparations contain an antimycotic or antiseptic in combination with an anti-inflammatory agent. In the treatment of skin infections accompanying onychomycosis, the following are used: Triderm, Travocort, Mikozolon, Pimafucort, Lorinden S, etc.
Azole, allylamine, morpholine compounds, as well as mixed group drugs are active against a large number of pathogens. Considering that quite often mycoses of the feet are caused by mixed fungal flora, it is preferable to prescribe these drugs, which are broad-spectrum antimycotics. Most of them damage the cytoplasmic membranes of fungal cell walls, suppressing the synthesis of their main components, in particular ergosterol.
Currently, the mycologist has highly effective systemic antimycotics: itraconazole (Sporonox, Orungal), fluconazole (Diflucan, Forkan), terbinafine (Lamisil), the antifungal effect of which is reflected in the table.
One of the important principles of topical therapy for mycotic skin lesions is the alternation of external antifungal drugs, which avoids resistance of dermatomycetes to them.
For squamous-keratotic forms of skin lesions, keratolytic agents are used as part of collodion peels or ointments: Arabian, Arievich, Andriasyan ointment or 5-10% Salicylic ointment. For candidal lesions, use Nystatin, Levorin, Amphotericin ointments, Pimafucin 1-2 times a day for 10-15 days. As a result of treatment, foci of candidal intertrigo, interdigital candidal erosions, and paronychia are resolved.
For acute skin mycoses with a pronounced inflammatory component, treatment begins with the elimination of swelling, hyperemia, exudation, eczematization, and allergic rashes. Lotions and wet-drying dressings with disinfectant and astringent compositions are prescribed: tannin, ethacridine, boric acid, etc. Then 2–5% boron-naphthalan paste, 5% ASD paste, as well as combinations of antifungal and corticosteroid agents in creams are used: Mycozolon, Travocort, Triderm. At the same time, acute inflammatory phenomena are quickly eliminated, which makes it possible to subsequently switch to treatment with fungicidal agents. It is recommended to use external agents with corticosteroids for 7–8 days to avoid activation of the mycotic process.
After acute inflammatory phenomena have subsided or after detachment of the stratum corneum in hyperkeratosis, azole antimycotic drugs can be used: Canesten, Clotrimazole, which are used 1 to 3 times a day, applying a thin layer to the lesions.
External dosage forms of terbinafine have high therapeutic activity: Lamisil (1% spray, cream), Lamisil Dermgel (gel). All forms have pronounced antimycotic and antibacterial properties. The presence of three dosage forms allows the mycologist to use the drug with the greatest benefit. Thus, Lamisil spray is indicated for acute mycoses with hyperemia, swelling, and rashes. The areas irrigated with the spray are covered with a thin film and isolated from the environment. Lamisil spray does not cause irritation and leads to a rapid resolution of mycosis areas: pain, itching, burning disappears, the lesions turn pale and dry out. With the help of Lamisil spray, foci of erythrasma are cured within 5 days. Within 7–10 days, recovery occurs in patients with various forms of lichen versicolor. Lamisil Dermgel, like the spray, is more indicated for acute mycoses, as it has a pronounced cooling effect and is easily applied to the affected areas. For erythematous-squamous and infiltrative manifestations of skin mycoses, the use of Lamisil in the form of a cream is indicated. The gel and cream of this drug are also effective for microsporia, lichen versicolor, candidiasis of large skin folds and periungual ridges. When using Lamisil cream for one week, a concentration of the drug is created in the skin that retains its fungicidal properties for another week after its discontinuation. This circumstance justifies short courses of treatment with Lamisil compared to other local antifungal agents.
Therapy for mycoses of the scalp, as well as in the treatment of smooth skin, is carried out with systemic and external antimycotics. Apply 2–5% tincture of iodine to the foci of mycosis and apply antifungal ointment in the evening. In cases of significant inflammation, combination drugs are used that contain, in addition to antimycotics, corticosteroid hormones. During an infiltrative-suppurative process, remove crusts with 2-3% Salicylic ointment and use disinfectant solutions (Furacilin, potassium permanganate). To increase the effectiveness of treatment, it is recommended to shave the hair on the head every 10 days.
I. V. Kurbatova , Candidate of Biological Sciences G. A. Plakhotnaya , Candidate of Medical Sciences
IMPiTM im. E. I. Martsinovsky, MMA named after. I. M. Sechenova
Tests and diagnostics
The diagnosis is made based on examination of the patient and laboratory data:
- Microscopy of material is a quick method of preliminary diagnosis. The materials used for laboratory examinations are hair, scales, skin scrapings, and crusts, which are taken from areas that have not been treated. Test preparations are pre-treated with potassium hydroxide (KOH, which is why the test is called a KOH test). With a microscopic examination, a laboratory technician can see and distinguish groups of fungi: dermatomycetes, yeast molds and yeast-like fungi. In scrapings, dermatophytes are represented by thin, straight and almost non-branching mycelium. M. furfur is detected as round cells (diameter 3–8 μm) that are collected in clusters, and curved banana-shaped mycelial hyphae can also be detected. Fungi of the genus Candida are represented by budding yeast cells and pseudomycelium in the form of a branching chain of cells. In most cases, lichen versicolor is diagnosed only by microscopy of the specimen, since culture of the material is often inconclusive.
- Cultural research - inoculation on a medium with subsequent identification of the species.
- For hair microsporia and pityriasis versicolor, an examination is carried out under the rays of a WOOD lamp - the lesions have a characteristic glow. With microsporia, the lesions have a bluish-green glow. With pityriasis versicolor, there is a copper-orange glow and even subclinical forms of infection are detected. The examination is carried out not only for primary diagnosis, but also to monitor the healing process.
Types of fungal skin infections
Depending on the pathogen, the symptoms of mycosis may vary slightly in each individual clinical case. In order to verify the preliminary diagnosis, additional tests are prescribed. During the latter, as a rule, the direct causative agent of the disease is identified. Subsequently, based on the data obtained, one of the following diagnoses is made:
- Trichophytosis (ringworm) - the causative agent of the disease is fungi of the genus Trichophyton. As the latter penetrates into the deep layers of the dermis, bright red spots appear on the patient’s facial skin. The affected areas peel off and become covered with multiple nodules.
- Pityriasis versicolor (varicolored) - the pathology is caused by the yeast-like pathogenic fungi Malassezia furfur. Against the background of the disease, the infected person develops pink scaly spots, which subsequently increase significantly and merge into a single pathological focus.
- Seborrheic dermatitis - this type of lesion occurs due to infection with fungi of the genus Malassezia furfur. Focal manifestations of this disease are located mainly in places of greatest accumulation of sebum. In some cases, pathological formations are covered with a hemorrhagic crust. Seborrheic dermatitis is accompanied by itching.
- Rubromycosis - the causative agent of this type of mycotic infection is fungi of the genus Malassezia rubrum. With this form of lesion, large red spots appear on the patient’s skin, surrounded by a ridge of papules.
- Microsporia – this type of mycosis is caused by Microsporum. The disease is characterized by large red spots, above which rises a ridge covered with multiple blisters.
- Candidiasis is caused by a yeast fungus of the genus Candida. Along with the skin, the pathogen can infect mucous membranes. Thus, painful blisters filled with serous fluid are often found not only on the skin, but also in the patient’s mouth.
In children
The main sources of infection of children with zoophilic fungi are stray cats and kittens. The latter are more susceptible to the disease because they have an imperfect immune system and a developed delicate undercoat, which is a breeding ground for microsporum. Microsporia in children is called “feline” lichen. The main contingent consists of children aged 5 to 14 years. The peak incidence occurs in August-October. Microsporia spreads quickly when the pathogen is introduced into schools, sports clubs and kindergartens. Infection from a sick child is possible through household items, a shared towel. The incubation period of zoonotic microsporia is 5-8 days. Anthropophilic pathogens of microsporia (M. ferrugineum) are transmitted through household items and from person to person.
A fungus on a child’s face manifests itself in small, coin-shaped, multiple lesions 1-2 cm in size. They tend to merge. Visually, these foci are difficult to distinguish from foci of trichophytosis . The difference is that with microsporia there are a larger number of foci, vellus hair, eyebrows and eyelashes are more often affected. Microsporidae can also occur - these are allergic rashes, like nodules.
Manifestations of anthroponotic microsporia are similar to superficial trichophytosis. The lesions have clear boundaries and merge, forming bizarre outlines. The primary elements in the lesions are bubbles or nodules, and the secondary elements are crusts. In the classic version, two lesions are formed in the shape of a “ring within a ring”.
Photo of a fungus on a child’s face
With microsporia and trichophytosis, lesions are often found on the head. These are large, round, scaly patches of baldness. The hair within the lesion is broken off and, with microsporia, protrudes several millimeters above the skin; with trichophytosis, it breaks off at the level of the skin and is visible as a black dot (“stump”). Inflammatory phenomena on the scalp are not expressed. Only bestial pathogens in some cases can cause an infiltrative-suppurative form, in which the lesion protrudes above the skin and is covered with purulent crusts. In case of complications, the child may be hospitalized. If the diagnosis of microsporia and trichophytosis is confirmed, the patient is isolated for 35 days. Contact persons during this period are examined by a doctor. The fireplace is disinfected.
Superficial bacterial skin infections
Folliculitis
- inflammation of the hair follicle: abscess around the hair, redness of the surrounding area.
Pemphigus of newborns
- a severe contagious disease when inflammatory blisters cover the baby’s entire body, forming crusts and ulcers.
Impetigo
- against the background of redness, painless blisters with cloudy contents appear. Then the blisters shrink to yellowish crusts, leaving erosions.
Impetigo often occurs in children and young women. Localization: face, under the hair of the head, limbs. When staphylococcus attaches, the crusts become greenish or bloody. The disease spreads quickly in communities. If you suspect it, you need to isolate the child and bandage the wound.
Prevention
- Prevention of skin candidiasis involves taking antifungal drugs with long-term or frequent use of antibiotics, hormones, and immunosuppressants. Taking antifungal drugs orally ( Natamycin , Fluconazole ) should continue throughout the main course of antibiotic treatment.
- For trichophytosis, which is transmitted by animals, it is important to carry out disinfection in the habitats of stray animals and treat sick animals. For trichophytosis, which is transmitted from sick children or adults, it is necessary to identify the source of infection, isolate it, and disinfect it in schools, kindergartens and hospitals.
- It is necessary to carefully examine the fur of pets for the presence of disease and promptly treat them.
- Avoid contact with stray animals.
- After playing with animals, you should wash your hands thoroughly.
- Improve the living conditions for children in health institutions and carry out regular disinfection.
- Carrying out disinfection measures in sports complexes, hairdressing salons, hotels and saunas.
- Mandatory processing of professional tools in hairdressing salons.
Treatment of bacterial skin infections
It should start from the early stages and be carried out under the supervision of a specialist. In some cases, local treatment with antibacterial ointments and wiping with antiseptics is sufficient. Widespread rashes, deep pyoderma, require the prescription of systemic antibiotics. In chronic cases, the doctor may recommend autohemotherapy and immune drugs.
Surgical treatment is carried out if the abscess does not open on its own or if a rough scar must be avoided. Laser coagulation and physiotherapy are used to restore tissue.
It is important to identify and treat concomitant diseases, eliminate adverse external effects on the skin, and select nutrition.
List of sources
- Kubanova A.A., Potekaev N.S., Potekaev N.N. Guide to practical mycology. – Moscow, Financial Publishing House “Business Express”, 200 p.
- Sergeev A. Yu., Sergeev Yu. V. Fungal infections. Guide for doctors. M.: BINOM-Press, 2003. 440 p.
- Clinical dermatovenerology. Guide for doctors in 2 volumes / Ed. Yu. K. Skripkina, Yu. S. Butova. M.: GEOTAR-Media, 2009. T. 1, 720 p. T. 2, 928 p.
- Potekaev N. S. Microsporia in adults / N. S. Potekaev, L. R. Plieva, S. V. Shkrebets // Clinical dermatology and venereology. - 2008. - No. 4. - P. 19–21.
- Sergeev Yu.V., Shpigel B.I., Sergeev A.Yu. Pharmacotherapy of mycoses. M.: Medicine for everyone, 2003. – 200 p.