Thigh lift surgery (femoroplasty) is less discussed than, for example, liposuction or a tummy tuck, but it is considered no less popular. The main patients of this operation are women who suffer from excess fat in the thighs and buttocks. Problems in this area are much more common among them than among men. A thigh lift has something in common with liposuction, as it gets rid of excess fat deposits, but its higher priority is the removal of excess skin.
A thigh lift can be considered as a way to remove excess fat and skin tissue, and also as one of the stages in the treatment of obesity (after bariatric surgery). Thigh lift is included in the complex of post-bariatric surgeries along with abdominoplasty, body lifting and tightening of the skin of the arms and face.
There are two main types of thigh lifts - internal and external. Both operations are different and are designed to solve different problems.
Best Candidate for External Thigh Lift
Priority for an internal thigh lift is given when the main problem area is excess fat and skin on the outer thighs and buttocks, i.e. what is called “thigh flaps” or “breeches”. This aesthetic problem is often faced by women with a pear-shaped figure.
As a rule, an external thigh lift is rarely performed independently; it is usually combined with an internal one.
An external thigh lift can be performed after one or more unsuccessful liposuction sessions, when too much fatty tissue has been removed, but the skin has not had time to recover and has begun to sag.
Conclusions.
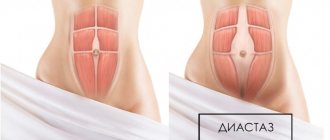
- The basic principle of new modifications of the medial thigh lift is the rigid fixation of the moving tissues of the thigh to the periosteum of the body and the branch of the pubic bone.
- The technology of moving and suturing the superficial fascia of the thigh with the periosteum of the pubic bone allows for the most durable fixation of the tissues of the inner surface of the thighs with minimal loss of correction of their position in the postoperative period.
- The modifications we have developed for medial thigh skin tightening allow us to obtain predictable and aesthetically acceptable results: postoperative scars are subject to minimal expansion and there is no dislocation to the thigh.
Best Candidate for Internal Thigh Lift
Internal thigh lift is more popular than external thigh lift, since problems usually lie on the inner thigh. The skin there is softer, fat accumulates more intensely, and as a result, many women suffer from sagging, loose skin on the inside of the legs and excess fat.
Problems can also appear in the absence of excess fat, for example, after severe weight loss, when the skin does not shrink, but begins to sag in folds on the legs like lowered stockings.
So, the best candidate for an internal thigh lift would be a patient with excess fat and skin tissue in this area. Such deficiencies can cause not only aesthetic discomfort, but also physical discomfort - when walking, irritation appears due to friction of the legs.
In general, it can be said that a thigh lift is suitable for people who have at least one of the following problems:
- Loss of skin turgor (decrease in elasticity and firmness) as a result of age-related changes;
- Excessive volumes of fat deposits in combination with inelastic skin;
- Excessively loose and weakened skin due to severe weight loss.
Lifting methods and their features
There are many techniques for restoring healthy skin on your legs. Most in demand:
- RF lifting - the skin is exposed to radio frequency radiation. Cells start the regeneration process and begin to produce collagen and elastin. The result is rejuvenation and improved tone.
- Thread lifting - the doctor outlines a mesh for hip correction and inserts threads along it under the skin. They reliably reinforce the problem area and tighten the skin.
- Mesotherapy is injections of drugs that deeply affect the skin and fat deposits. They have a visible and lasting effect.
- Aikun laser - infrared radiation has a targeted effect on the skin and stimulates cell renewal, improves the quality of the skin, and tightens it.
- Laser rejuvenation is a laser technique aimed at combating increased skin sagging.
- Fractional thermolysis is the effect of a laser pulse on the skin, which stimulates skin renewal and increases its elasticity.
- Biomodeling Profhilo - injections of long-acting filler based on hyaluronic acid of different densities. Rejuvenate and tighten the skin.
- Introduction of fillers - preparations based on hyaluronic acid moisturize the skin and increase its elasticity.
Incision options for external thigh lift
External thigh lift is difficult to model. The doctor needs to simulate the new position of the fat and skin tissues so that asymmetry does not occur.
External lifting begins with liposuction. After removing the fatty tissue, we proceed to excision of excess skin. The incision, called a lateral incision, is made from the groin line up around the thigh near the pelvic bone so that the scars are subsequently hidden under underwear. If the volume of tissue to be removed is quite large, the incision passes under the gluteal fold.
General recommendations
- Be sure to take time to warm up before and after playing sports, this will help avoid injuries and protect the body from unnecessary stress.
- One of the keys to success is regular training. To keep yourself in good shape, a few workouts a week are enough, but to lose weight and combat problem areas, you need more frequent and intense exercise.
- Equally important is the correctness of the exercises. Give them special attention.
- If possible, do a light massage or scrub after class. A comprehensive fight against excess weight is always better than a targeted one.
Incision options for internal thigh lift
The incision to eliminate excess on the inner thigh is called medial. The surgical field in this case is located in the perineum. The area of excised skin starts from the groin area, goes down vertically, and then rises, ending at the fold under the buttock. Thus, the flap of excised skin forms a triangle or T-shape. The latter is done when it is necessary to remove a lot of tissue. In the case, for example, when the patient has large excess skin to remove. As a result of the T-shaped incision, a scar of a similar shape is formed. The triangular incision is sewn together with a single suture, which runs from the crease under the buttocks to the groin area.
Diagnostics
Making a correct diagnosis is the key to effective and high-quality treatment. Therefore, there is a certain examination algorithm, the scope of which can be determined by the doctor. The patient's diagnostic path consists of the following steps:
1. Consultative examination and history taking.
2. Manual muscle testing, assessment of motor stereotypes, identification of violations of the biomechanical chain of the musculoskeletal system.
3.Performance of specific tests and samples by the patient
4.Complete additional laboratory and instrumental research methods: general and biochemical blood tests, laboratory tests for specific markers, radiography, ultrasound, electroneuromyography, MRI, MSCT.
- Consultation with doctors of related specialties to verify differential diagnosis.
This scope of diagnostics makes it possible to accurately determine the pathology and cause that caused the pain, since pain in the hip, buttock, and groin area can have different etiological factors. A well-constructed diagnostic strategy allows the doctor to prescribe the necessary range of therapeutic measures in a short time.
How noticeable will the scars be after a thigh lift?
Many surgeons note that after a thigh lift, problems may arise with narrowing of the perineum and sutures coming apart. The reasons for this lie in the fact that the legs are a moving part of the body. While walking, the scars constantly rub against the perineum. In addition, they are more affected by gravity and the weight of the upper body.
Today, in order to prevent scars from spreading, the formation of unaesthetic scars and narrowing of the perineum, doctors use special skin stitching techniques. This is one of the key questions. In particular, the technique of rigid tissue fixation with sutures to the bone fascia is used. In this case, biodegradable threads are used, which help create connective tissue inside, keeping the sutures from resorption.
In addition, this “rigid attachment” helps eliminate vulvar enlargement, a common complication after a thigh lift that can lead to infection.
As a result, we can say that modern wound suturing methods reduce the risk of suture expansion. Patients must adhere to the regimen and wear compression garments. Usually the restriction on wearing underwear is lifted a month after the operation, but surgeons recommend not putting off compression hosiery too far, but still wearing it periodically. It helps the skin “breathe correctly”, increases blood flow, is responsible for the supply of oxygen to the muscles, and generally improves the condition of the skin of the legs and prevents post-operative scars from growing.
You can learn more about this operation in the “Thigh Lift” section.
Introduction
Among the entire range of operations aimed at correcting body contours, medial thigh lift occupies a very modest place.
While studying the literature, we found extremely scant coverage of this topic in monographs and on the pages of specialized periodicals. First of all, this is due to the dissatisfaction of both patients and surgeons with the results of the operation - under the influence of gravity, the work of muscles and joints, postoperative scars stretch and “slide” onto the thigh from the femoral-perineal groove. Patients experience both cosmetic problems - the scar appears in the visible zone, and functional ones - the perineum expands, up to the complete smoothing of the femoral-perineal grooves. Meanwhile, in our daily practice, we regularly encounter patients who have: a) an age-related decrease in skin turgor, b) who wish to reduce the volume of the upper third of the inner thighs using liposuction, c) who have pronounced relaxation of the skin of the thighs after severe weight loss. Under these conditions, only tightening the skin of this area in a vertical direction with the removal of its excess can eliminate the existing problems. It is known that for this purpose, back in the middle of the 20th century, surgeons simply excised excess skin and sutured its edges. The deterioration of the results of the operation over time (stretching of scars and their dislocation to the thigh) led to an improvement in the technique of its implementation. So, since 1988, in addition to the skin suture, it was proposed to place additional deep sutures between the dermis, and subsequently the superficial fascia of the thigh on the lateral side, and the Colles fascia on the medial side. (The fascia of the Wheel is the deep inner layer of the superficial fascia of the perineum, which is located behind the border of the urogenital diaphragm. It starts from the branches of the ischium and pubic bones and continues anteriorly and upward to the abdominal wall) (Fig. 1).
|
This option of tissue fixation during a medial thigh lift is still considered classic to this day. However, evaluating these operations based on rare publications of clinical observations, seeing patients who had previously had a thigh lift using known technologies in other medical institutions, the fact of dissatisfaction with long-term aesthetic results turned out to be quite obvious to us (Fig. 2a, b).
| |
All this forced the team of authors to look for a way to more reliably connect tissues.
Understanding that the deep suture of the thigh tissue to the fascia of the Wheel does not provide a strong fixation and is subject to stretching over time with all the ensuing consequences, led us to the idea that the mobile tissue of the thigh must be connected to a completely immobile structure. And such an anatomical unit in this zone is only the pubic bone. In 2001, at the GrandMed clinic, a technique for fixing the superficial fascia of the thigh to the periosteum of the body and the branch of the pubic bone was developed and began to be successfully used, which allowed us to achieve guaranteed good long-term results in the first years of its use (Fig. 3).
|
A new modification of tissue tightening of the inner thighs was first presented to the surgical community in the form of a report at the “Fourth Congress on Plastic, Reconstructive and Aesthetic Surgery with International Participation”, held in Yaroslavl in June 2003.