There are contraindications. Specialist consultation is required.
Indications Contraindications Preparation Types of operations Rehabilitation
Colporrhaphy is a vaginoplasty performed when the vagina is stretched and the uterus prolapses after childbirth or with age.
Levatoplasty is an operation performed on the muscles of the perineum to restore the pelvic floor. It allows you to strengthen the back wall of the vagina and return the genitals to the pelvis.
These two techniques can be combined, that is, levatoroplasty can be performed in conjunction with colporrhaphy in case of severe stretching of the vaginal walls or if connective tissue scars are present on them after ruptures.
Indications for colporrhaphy surgery
Colporrhaphy refers to vaginal plastic surgery. The operation of colporrhaphy is the suturing of the vaginal walls when they expand, prolapse and prolapse.
Symptoms of vaginal dilatation and prolapse:
- Disturbances in intimate life, when a woman does not feel anything during sexual intercourse
- Pain when tense abdominal muscles
- Discomfort and unpleasant sensations in the vagina, feeling of a foreign object
Degrees of vaginal prolapse:
- Mild (prolapse of the vaginal walls, which may not interfere with sexual activity, and also does not cause harm to health)
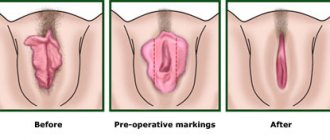
- Moderate (prolapse of the mucous membrane outward - in appearance it resembles a “rose” dangling in the perineum). Constant contact of the mucous membrane with underwear and its insufficient hydration leads to thinning and the appearance of cracks through which bacteria can penetrate, causing inflammatory processes.
- Severe (prolapse of the uterus or cervix). With this degree, the patient can hardly move, urinary incontinence appears, urination itself is difficult, pain appears in the lower abdomen and in the bladder area. With this form, colporrhaphy surgery is no longer cosmetic, but vital.
Causes of vaginal prolapse and expansion:
- Difficult birth (with ruptures)
- Pelvic organ injuries
- Chronic constipation (if a woman constantly pushes, straining her abdominal muscles)
- Reduced estrogen levels in the body (this is usually characteristic of mature women)
- Sedentary lifestyle
In all these cases, the operation colporrhaphy is indicated, which consists of removing the excess (prolapsed) vaginal wall (anterior or posterior) and correcting the external opening. After excision, the vaginal muscles are tightened and sutured.
Types of colporrhaphy:
- Front
- Rear
- Median (Lefort-Neugebauer operation)
With anterior colporrhaphy, the anterior wall of the vagina is sutured; with posterior colporrhaphy, the posterior wall is sutured. The median one covers all areas of the vagina and is performed mainly only on older women suffering from complete prolapse of the uterus and who are no longer sexually active.
The surgeon determines the degree of vaginal prolapse during examination in a resting position and, separately, in tension. After this, a decision is made on the type of colporrhaphy that is required to eliminate the problem. If vaginal prolapse is accompanied by uterine prolapse and urinary incontinence, multiple surgeries may be needed.
The operation is performed under general anesthesia or spinal anesthesia. Previously, the patient undergoes a full medical examination, including:
- Consultations with a gynecological surgeon and anesthesiologist
- Gynecological smear
- Blood test for sexually transmitted diseases
- General blood analysis
- Blood chemistry
- Blood clotting test
Postoperative period
The length of hospitalization depends on the extent of the surgical intervention and the characteristics of the postoperative period. In some clinics, posterior colporrhaphy is performed according to the principle of “one-day surgery”; the patient is sent home 4 hours after the operation. The suture material used in posterior colporrhaphy to restore the integrity of the vaginal wall dissolves on its own within 6 weeks. Perineal sutures made of non-absorbable thread are removed after 14 days.
For 6-8 weeks, the patient must strictly observe sexual rest. For 7 days after posterior colporrhaphy, you are not allowed to sit at a right angle; for 2 weeks you are not allowed to squat. After each use of the toilet, it is necessary to wash the perineum with an antiseptic solution. To prevent inflammatory processes, antibacterial therapy and vaginal sanitation with complex antimicrobial and antifungal suppositories are prescribed for 5-7 days. In the early postoperative period, dysuric disorders (reaction to the urinary catheter), tissue swelling, and bloody vaginal discharge may be observed. A follow-up examination on a gynecological chair after posterior colporrhaphy is carried out a week later. When returning to sexual activity, it is necessary to use lubricants for the first time.
Contraindications for surgery
Contraindications to colporrhaphy surgery can be relative or absolute.
Relative contraindications include age under 18 years, but this prohibition only applies to aesthetic colporrhaphy. If colporrhaphy is required by functional abnormalities in the functioning of organs and medical indications, then the operation is performed at any age, even early.
Other contraindications for surgery:
- Venereal diseases
- Chronic inflammatory processes
- Acute thrombophlebitis
- Heart failure
What tests and examinations should you undergo in preparation for colporrhaphy?
The list of necessary examinations is prescribed by the doctor after a preliminary consultation and examination. The list of mandatory diagnostic procedures includes:
- smear on the flora and cleanliness of the vagina;
- blood test to determine Rh factor and group;
- clinical and biochemical blood examination;
- examination for STDs, hepatitis, human immunodeficiency virus, syphilis;
- fluorography.
When preparing for surgery, a woman needs to consult an anesthesiologist and therapist. According to indications, consultations with other specialists are prescribed.
Thanks to a comprehensive examination, the doctor can identify possible contraindications to vaginoplasty, determine the technology and procedure for the operation.
Rehabilitation after surgery
The colporrhaphy operation itself lasts very little - from 30 to 60 minutes, and is well tolerated by women. However, this is a serious surgical intervention, and after it the patient will have to undergo a full rehabilitation period.
For the first 2-3 days after colporrhaphy, the patient remains in the hospital under the supervision of doctors. Then the woman can return home, but for another two weeks she is only allowed to take a horizontal position - sitting is strictly prohibited.
During rehabilitation after colporrhaphy surgery, the patient is prescribed a course of antibiotics and painkillers - as with a standard operation. At the same time, it is recommended to undergo physiotherapeutic procedures, wear supportive compression garments, a bandage, and engage in light physical therapy as recommended by a doctor.
During the rehabilitation period (2 months) after colporrhaphy it is strictly prohibited:
- Have sexual intercourse of any kind
- Play sports or any physical activity
- Lifting weights
- Tighten your abdominal muscles
Who should undergo vaginal reduction surgery: a plastic surgeon or a gynecologist?
In 2022, changes were made to Order No. 298n “On approval of the Procedure for the provision of medical care in the field of Plastic Surgery”, which indicated the “area of work” of a plastic surgeon; it clearly defined that a plastic surgeon cannot perform operations on the internal genital organs
, which includes the vagina.
A plastic surgeon can only perform operations on the external genitalia (labiaplasty), nothing more. Therefore, today this operation should be performed only by gynecological surgeons
.
Anterior colporrhaphy
Anterior colporrhaphy is plastic surgery of the anterior vaginal wall.
Indications for anterior colporrhaphy:
- Prolapse of the anterior vaginal wall
- Prolapse and prolapse of the anterior vaginal wall along with the posterior wall of the bladder
Anterior colporrhaphy surgery technique:
- An extra section of mucous membrane is isolated on the anterior wall of the vagina
- This area is excised
- Deep sutures are applied
- A continuous suture connects the edges of the vaginal mucosa
Navigation:
- More details
- The main thing you need
- Anterior colporrhaphy
- Posterior colporrhaphy
- Median colporrhaphy
- Recovery period
- How much does colporrhaphy cost?
- with age or after childbirth, severe stretching of the vagina occurred, and the elasticity of the walls decreased significantly;
- prolapse or (even worse) prolapse of the vaginal walls, cervix or uterus itself has occurred;
- there are congenital anomalies of the vagina;
- urinary incontinence;
- protrusion of the pelvic floor organs into the walls of the vagina (urethra, bladder, rectum);
- discomfort, pain during sexual intercourse;
- inability to experience orgasm, decreased (or absent) sexual pleasure.
Where do all these “troubles” come from? Of course, the main reason for the appearance of unfavorable changes is pregnancy and childbirth, especially when the fetus is large or multiple pregnancies, multiple births. In “second place” is age - it is quite natural that with age the elasticity of the vagina is lost, dryness, itching appears, the external genitalia become flabby and aesthetically unattractive. Also, a woman’s intimate health is influenced by factors: constant standing, heavy physical labor, and inappropriate sexual preferences. Another reason that is “gaining momentum” is general atony (nowadays fashionable exhaustion, in which uterine prolapse occurs due to the almost complete absence of the muscular frame).
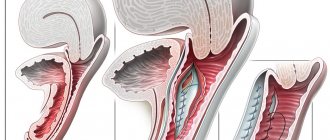
Posterior colporrhaphy
Posterior colporrhaphy (colpoperineorrhaphy) is plastic surgery of the posterior vaginal wall.
Indications for posterior colporrhaphy:
- Prolapse and prolapse of the posterior wall of the vagina, caused by ruptures of the perineum (during childbirth), decreased tone of the peripelvic tissues
- Threat of uterine prolapse
- Rectal hernias
Posterior colporrhaphy surgery technique:
- A triangle is separated on the back wall of the vagina
- Within this triangle, the mucous membrane is cut off
- The levators are exposed and connected with catgut sutures
- Several separate stitches are placed between them
- The membrane of the posterior surface of the vagina is sutured with a continuous suture.
conclusions
1. When comparing the results of the two surgical aids, it becomes obvious that both techniques provide satisfactory functional results, but each has a number of disadvantages and advantages. A higher risk of recurrence of genital prolapse and the occurrence of long-term mesh-associated complications indicates the need to improve the materials used and the methods of their fixation in tissues. At the same time, the disposition of the walls of the vagina and adjacent organs, created during Neugebauer-Lefort colporrhaphy, increases the risk of developing stress incontinence.
2. Individual choice of surgical treatment, taking into account the age and degree of sexual activity of the patient, assessment of risk factors for the development of certain complications, as well as an accessible explanation to women of the nature and scope of the upcoming treatment help reduce the number of complications and achieve the best results in the treatment of genital prolapse.
The authors declare no conflict of interest.
Median colporrhaphy
This operation is performed for complete prolapse of the uterus, mainly only for older women who are no longer sexually active. Since the complications of median colporrhaphy are the inability to have sexual intercourse in the future and the lack of access to the cervix for examination. Therefore, before median colporrhaphy, an examination is required to exclude the patient’s predisposition to cervical cancer.
Technique of median colporrhaphy surgery:
- The anterior and posterior lips of the cervix are grabbed with forceps, removing them together with the vagina from the genital slit.
- Equal sections of the mucous membrane are cut off from the anterior and posterior walls of the vagina.
- Sutures are used to connect the front edges of the wound first, then the side and back edges.
- The cervix is immersed into the vagina.
- There are channels left and right for the outflow of secretions from the uterus.
Material and methods
The study included 41 patients who underwent surgical treatment in the period from 2010 to 2012 in the departments of operative gynecology and endoscopic surgery of the Moscow Regional Research Institute of Obstetrics and Gynecology (Table 1). The results of the operations were assessed 2-4 years after surgical treatment. This period, in our opinion, is optimal for assessing the long-term results of surgical treatment [8, 10—12].
Table 1. Characteristics of the examined groups of patients
Group 1 included 21 patients who underwent vaginal extraperitoneal colpopexy with simultaneous use of synthetic prostheses of the Prolift + M anterior and posterior system; Group 2 included 20 patients who underwent median colporrhaphy using the technique proposed by Lefort and Neugebauer.
The follow-up data of all patients, their complaints at the time of the study and genital status were studied. If necessary, women underwent additional studies (ultrasound of the pelvic organs, urine culture, complex urodynamic study), as well as consultations with related specialists (urologist, neurologist, coloproctologist).
To assess the subjective attitude of patients to the results of their surgical treatment, a specialized urogynecological questionnaire PFDI-20 was used [13], which was filled out by 18 patients from the 1st group and 17 from the 2nd group during the control examination. This questionnaire includes 3 blocks of questions that allow you to assess the severity of symptoms of genital prolapse, urination and defecation disorders on a 5-point scale.
Processing of the obtained data was carried out using parametric and nonparametric statistics methods. The differences are statistically significant at p
≤0,05.