There are several techniques for performing a forehead lift. Let's take a closer look at them. – coronary forehead and eyebrow lift; – endoscopic forehead and eyebrow lift; – temporal brow lift; – brow lift with an incision above the eyebrow; – transpalpebral fixation of the eyebrow (fixation of the eyebrow through the upper eyelid); – transpalpebral excision of the muscles of the nose (excision of the muscles of the glabella through the upper eyelid).
Coronal forehead lift
An open coronal forehead (brow) lift is performed through an incision at the top of the head from ear to ear and provides access to the anatomical structures of the forehead. After performing all surgical manipulations with the muscles, the surgeon removes excess skin (a strip of scalp about 1-2 cm) and applies sutures. Although this technique may seem scary, it is the oldest and most reliable method of surgical forehead rejuvenation.
The advantages of a coronary forehead and eyebrow lift are: long-term preservation of the results of the operation; absence of visible marks (due to the placement of incisions in the scalp, the scars become invisible after healing); can be performed on almost all patients (however, if you are a person with receding hairline, then you should give preference to an endoscopic forehead lift).
The coronal forehead lift is a highly invasive procedure. Although the surgery can be performed on anyone, we believe that only those patients who are not suitable candidates for an endoscopic forehead and brow lift will be candidates. In all other cases, we strongly recommend the latter.
There are many disadvantages of a coronary facelift: numbness in the upper part of the head for 6 months; A coronal forehead and eyebrow lift raises the hairline, which can be a problem for people with high foreheads who wear their hair back; high invasiveness of the operation; long period of rehabilitation, massive blood loss; risks of complications (scar formation, bald patches).
Despite the fact that open coronal forehead and brow lift is the “gold standard”, this technique is becoming outdated. Unfortunately, there are not many clinics in Moscow where high-tech, low-invasive endoscopic forehead lift is performed, which in its results is not inferior to the classics, and is many times superior in safety. At US Clinic, forehead lifts are performed only using advanced endoscopic technology.
Rehabilitation period after Brow lift
During brow lifting using an endoscopic instrument, a minimal number of nerve endings, blood vessels and hair follicles are affected. Therefore, the rehabilitation period is much shorter than after alternative methods of surgery. Recovery takes 3–4 weeks. Swelling and bruising completely disappear within 1–2 weeks. During the first week, it is forbidden to apply any cosmetics to the correction area, wash your hair, dry your hair with a hairdryer, or bend down sharply. Throughout the entire rehabilitation period, it is necessary to exclude visiting the bathhouse, sauna, swimming pool, solarium and physical activity.
Endoscopic forehead and eyebrow lift
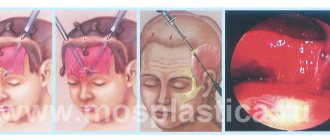
Endoscopic forehead and eyebrow lifting is performed through small incisions (up to 2 cm) behind the hairline using an endoscope (a special instrument with a tiny camera at the end). Monitoring his actions with a micro-video camera, the surgeon peels away the forehead tissue, cuts the ligaments and small muscles that form wrinkles, raises the eyebrows and fixes the tissue in a new position. The use of endoscopic technology gives complete control over the operation and high precision of execution. Thanks to good visualization of nerves and small blood vessels, their damage during surgery is eliminated, which reduces the amount of blood loss and the risk of complications.
Endoscopic forehead and brow lift is suitable for almost everyone, with the exception of patients with a very high forehead, thick or deep forehead wrinkles, severe drooping of the eyebrows and large excess skin in the eyebrows and glabella. Endoscopic forehead lift is an ideal option for bald or balding men who cannot hide the signs of surgery with hair or makeup.
The advantages of endoscopic forehead and eyebrow lift are obvious: reduced operation time compared to coronary forehead lift (about 1 hour); minimal invasiveness and short recovery period; absence of visible scars and severe complications; high efficiency of results, not inferior to an open forehead lift.
drawback to endoscopic forehead lift: the higher cost of the operation due to the high cost of endoscopic equipment.
Unfortunately, there are currently very few clinics that practice endoscopic forehead and eyebrow lifting, due to the lack of endoscopic equipment and experienced surgeons proficient in the technique.
Endoscopic forehead lift using bioabsorbable implants for tissue fixation
The endoscopic method of eyebrow lifting has easily won the sympathy of both plastic surgeons and their patients. The method allows for successful results and is less traumatic compared to traditional coronary lift and is associated with less swelling and numbness in the postoperative period, a shorter recovery period and the ability to better hide surgical scars. All this stimulates the development of new tools and concepts that would make endoscopic lifting even safer and more reliable. At the same time, controversy continues over the preservation of the effect of endoscopic eyebrow lifting in the long term. Many experts agree that the most important factors for achieving a lasting result are complete periosteal release, complete transsection of the muscles in the glabellar region and adequate effective fixation of the forehead tissues in a new, elevated position.
The endoscopic forehead lift method was first described by Vasconez et al in the early 1990s. The dissection was performed in the subgaleal plane and included dividing the procerus and corrugator muscles and making incisions into the frontal belly of the occipitofrontal muscle. The authors briefly touched on techniques for fixing the tissues of the forehead and eyebrows. The literature describes various methods of tissue fixation, including using permanent or absorbable screws, plates and nails, Kirschner wires, external cotton-gauze dressings, tension sutures, cortical tunnels and recesses with sutures of surgical adhesives, as well as techniques that do not providing for fixation. The amount of flap lift achieved with endoscopic lifting is the same as with coronary lifting. Therefore, in order to avoid subsequent eyebrow drooping, it is extremely important to ensure tissue fixation at several points. Most techniques described in the literature involve fixing the tissue being lifted at only one point. This type of fixation is associated with the “cheese-cutting effect”, where the suture material can cut through the tissue and thereby reduce the reliability of the brow lift. In this article, the authors describe their own experience in the use of bioabsorbable mini-endoprostheses, which provide tissue fixation at several points and thereby contribute to the dispersal of stress over a larger area.
METHODS ASSESSMENT
AND POSITIONING OF PATIENTS
The shape and asymmetry of the eyebrows in patients was assessed “in a standing position.” The surgeon manually raised the eyebrows and noted their position relative to the supraorbital margin. The supraorbital foramen was palpated and the trajectory of the supraorbital nerve was marked. At a distance of 1 cm medial to the supraorbital nerve, the trajectory of the supratrochlear nerve was marked (Fig. 1)
. The patient was placed on the operating table in the reverse Trendelenburg position with a slight tilt of the table, the hair was tied into bundles and removed from the surgical field.
ANESTHESIA
The operation is usually performed under intravenous sedation with the administration of a local anesthetic. After intravenous administration of a sedative, local injections of a solution containing equal parts (50/50) 2% bupivacaine with epinephrine 1:200000 and 2% lidocaine hydrochloride with epinephrine 1:200000 were performed to block the supraorbital and supratrochlear neurovascular bundles and anesthesia the frontal flap and tissue in the places of proposed incisions. The patient was then prepared for surgery and draped according to routine practice.
SECTIONS
At a distance of 2 cm above the hairline, a series of 4 incisions (12-14 mm long) (2 paramedian and 2 temporal) were made using a high-frequency scalpel. Paramedian incisions were made along a line parallel to the supratrochlear vessels down the calvarium. Temporal incisions crossed a line from the lateral nasal cartilage to the outer corner of the eye and were made to the deep temporal fascia.
DISCUT
Through the temporal incision, a dissection was made along the top of the superficial layer of the deep temporal fascia, which extended to the temporal line anteriorly and along the superior and lateral edge of the orbit and the zygomatic arch inferiorly. Through a paramedian incision, a periosteal dissection was performed downward to a distance of up to 1 cm from the supraorbital margin and glabella. The temporal recess was connected to the subperiosteal recess along the temporal line. At this point, a 5-mm 30-degree endoscope was inserted to visualize the rest of the incision. A Ramirez dissector was used to cut the periosteum below the lower part of the forehead to the level of the supraorbital rim. The trajectory of the supratrochlear and supraorbital nerves was determined and measures were taken to preserve them. Using a Ramirez nerve dissector, the periosteum was excised on both sides of the supratrochlear and supraorbital nerves along the entire arcus marginalis.
MUSCLE SEPARATION
Medial to the neurovascular bundles, the corrugator muscle and the procerus muscle were identified. The muscles were cauterized and separated using a high-frequency cutting cautery. The forehead tissue was then manually lifted to confirm its complete release from its attachment to the orbital margins.
FIXATION
First, the eyebrow was fixed lateral to the temporalis fascia. A 2-0 polyester-based braided suture was placed through the incision line through the skin as close to the eyebrow as possible. The placement is usually done just anterior to the hairline to relieve tension along the cut line and reduce the likelihood of alopecia. Using a scalpel with a No. 15 blade, a small stab incision was made through the epidermis. The suture material was passed back through this stab incision and secured to the temporalis fascia.
Tissue fixation was then performed at the midline using Endotine Foreheads (Coapt Systems Inc, Palo Alto, CA). Using a hand or low-power electric drill with a drill for forming a bone bed for endotin and a chuck, two monocortical holes were formed at the anterior edge of 2 paramedian incisions (Fig. 2 and Fig. 3)
.
A drop of octyl-2-cyanoacrylate (ISO-DENT; Ellman International, Oceanside, NY) was placed in each hole. Using the mini-endoprosthesis inserter supplied with the Endotine Forehead, the 3.0 mm spiked products were inserted into the holes so that they fit snugly against the outer plate of the cranial bone (Figure 4 and Figure 5)
.
The scalp was pulled up in the cranial direction for fixation on the pins of the mini-endoprosthesis (Fig. 6)
.
By pressing with a finger, the periosteum was fixed on the spikes of the mini-endoprosthesis (Fig. 7). To manufacture the Endotine Forehead mini-endoprosthesis, a bioabsorbable copolymer of lactic and glycolic acids is used. 6-12 months after implantation, complete resorption of the product occurs. The incisions were sutured with staples, and a Kerlix (Tyco Healthcare Group LP, Mansfield, Mass.) and Coban (3M Healthcare, St. Paul, Minn.) pressure dressing was applied to the forehead and removed after 24 hours.
POSTOPERATIVE CARE
The staples were removed 7-10 days after surgery. Patients could feel the mini-endoprosthesis for several weeks after the procedure. Feeling some numbness at the incision site is not unusual.
RESULTS
Since the authors began using the Endotine Forehead in March 2003, endoscopic brow lifting has been performed on 53 patients. A satisfactory rejuvenation effect in the forehead area was achieved in all patients, with the exception of one. This patient experienced repeated ptosis of the lateral end of the eyebrow, and therefore she required only lateral temporal fixation. The installed endotin provided a lasting effect of raising the eyebrows in the medial part.
Before the authors began using endotins for tissue fixation during endoscopic brow lift, the revision rate was 10%. In Fig. 8, 9 and 10 show photos of patients before and after endoscopic brow lift using endotin mini-endoprostheses for tissue fixation.
C O M M E N T A R I I
Permanent fixation of the eyebrow is ensured by the healing of the periosteum to the skull bone at a new, higher point. Data from recent studies indicate that complete healing of the periosteum in a new location occurs within 2 weeks after surgery (Fig. 18, 19). According to Romo et al (Fig. 20) and Sclafani et al (Fig. 21), engraftment requires 6 to 12 weeks. Numerous methods have been described for fixing soft tissues until the periosteum takes root in a new location. The inability to provide long-term fixation when using external compression bandages and techniques that involve moving a skin flap leads to unpredictability of lifting results. Rigid fixation techniques using permanent and absorbable fixing elements are more reliable and allow for a more lasting tightening effect.
The method of tissue fixation using Endotine Forehead mini-endoprostheses is safe, simple, effective and reliable. The advantages of using endotins include the absence of the need for the use of metal screws protruding above the surface of the scalp, which can cause irritation in the wound and alopecia, for sutures, which can puncture the hair follicles, which can also lead to alopecia, as well as removal of fixing elements, since endotins dissolve on their own over time. Thanks to the unique design of the mini-endoprosthesis, tissue fixation is ensured at several points, due to which stress is distributed over a larger area rather than concentrated at one point. If asymmetry is detected in the postoperative period, soft tissue fixation can be adjusted to improve the aesthetic result.
Fixation techniques that concentrate stresses from suspended tissue in the scalp incision area create the potential for alopecia. Attaching endotin to the calvarium eliminates unnecessary tension on the scalp. The hole in the bone pre-formed by the cutter has a depth of 3.95 mm, which eliminates accidental intracranial damage that is possible when using the technique of fastening through the recesses in the bone of the cranial vault and the bridging technique.
Possible complications with the use of mini endotin endoprostheses include failure of the device, the need for repositioning due to asymmetry, and the patient's perception of a foreign body in her head. Patients with thin skin can palpate the implanted product until it dissolves. The skin covering the mini-endoprosthesis is often painful. In addition, the use of endotins increases the cost of the lifting procedure, since the cost of one product is higher. In conclusion, it should be noted that the use of Endotine Forehead mini-endoprostheses is a safe, simple and effective method of fixing the forehead tissue after a brow lift. The product does not need to be removed; it provides stress distribution over a larger area and the possibility of correction in the postoperative period.
REFERENCES
1. Puig CM, LaFerriere KA.
A retrospective comparison of open and endoscopic brow-lifts.Arch Facial Plast Surg. 2002;4:221-225. 2. Koch RJ. Endoscopic browlift is the preferred approach for rejuvenation of the upper third of the face. Arch Otolaryngol Head Neck Su.rg2001;127:87-90. 3. Vasconez LO, Core GB, Gamboa-BobadillaM. Endoscopic techniques in coronal brow-lift.Plast Reconstr Surg. 1994;94:788-793. 4. Vasconez LO. The use of the endoscope in brow-lifting. Video presented at: American Society of Plastic and Reconstructive Surgeons annual meeting; September 1992; Washington, DC. 5. Rohrich RJ, Beran SJ. Evolving fixation methods in endoscopically assisted forehead rejuvenation: controversies and rationale. Plast Reconstr Surg. 1997; 100:1575-1582. 6. Landecker A, Buck JB, Grotting JC. A new resorbable tack fixation technique for endoscopic brow-lifts.Plast Reconstr Surg. 2003;111:880-886. 7. Pakkanen M, Salisbury AV, Ersek RA. Biodegradable positive fixation for the endoscopic brow-lift.Plast Reconstr Surg. 1996;98:1087-1091. 8. Chasan PE, Kupfer DM. Direct K-wire fixation technique during endoscopic brow-lifts.Aesthetic Plast Surg. 1998;22:338-340. 9. KimSK. Endoscopic forehead-scalp flap fixationwith K-wire. Aesthetic Plast S.urg 1996;20:217-220. 10. Matarasso A. Endoscopically assisted forehead-brow rhytidoplasty: theory and practice. Aesthetic Plast Surg. 1995;19:141-147. 11. Smith DS. A simple method for forehead fixation following endoscopy [letter]. Plast Reconstr Surg. 1996;98:1117. 12. Ramirez OM. Endoscopic techniques in facial rejuvenation, I: an overview.Aesthetic Plast Surg. 1994;18:141-147. 13. Kobienia BJ, Van Beek A. Calvarial fixation during endoscopic brow-lift.Plast Reconstr Surg. 1998;102:238-240. 14. McKinney P, Sweis I. An accurate technique for fixation in endoscopic brow-lift: a five-year follow-up.Plast Reconstr Surg. 2001;108:1808-1810. 15. Jones BM, Grover R. Endoscopic brow-lift: a personal review of 538 patients and comparison of officio techniques. Plast Reconstr Surg. 2004;113:1242-1250. 16. Marchac D. Use offi brin glue in forehead-lifts. Paper presented at: Emory Aesthetic Surgery/Endoscopy International Symposium; September 1995; Atlanta, Ga. 17. Koch R, Troell RJ, Goode RL. Contemporary management of the aging brow and forehead.Laryngoscope. 1997;107:710-715. 18. Kim JC, Downs JC, Azuola ME, Graham D. Time scale for periosteal readhesion after brow-lift. Laryngoscope. 2004;114:50-55. 19. Kriet JD, Yang CY, Wang TD, Cook TA. Evaluation of pericranial skull adherence during healing in the rabbit model. Arch Facial Plast Surg. 2003;5:67-69. 20. Romo T, Sclafani AP, Yung RT, et al. Endoscopic foreheadplasty: a histologic comparison of periosteal refixation after endoscopic versus bicoronal lift. Plast Reconstr Surg. 2000;105:1111-1117. 21. Sclafani AP, Fozo MS, Romo T, McCormick SA. Strength and histological characteristics of periosteal fixation to bone after elevation. Arch Facial Plast S. urg 2003;5:63-66.
Temporal brow lift
A temporal (lateral) brow lift is aimed at eliminating wrinkles in the outer corners of the eyes and lifting the outer ends of the eyebrows. Surgical incisions are made in the temporal areas of the scalp. Ideal for patients with limited signs of aging of the forehead skin who require lifting of only the outer edge of the eyebrow without drooping of the inner part.
Temporal lift cannot be used to correct forehead wrinkles. A lateral brow lift is often performed on bald men or on patients who want to “touch up” a previous brow lift. Read more about temporal brow lift.
What is browlifting and do you need it (marieclaire.ru)
We understand all the nuances of one of the most popular plastic surgeries today, the effect of which, according to surgeons and patients, is comparable to a circular facelift.
When it comes to correcting the eyebrows and the area of the face above them, as a rule, there is no limit to perfection: even with the help of numerous procedures, you are unlikely to get the very result that you pictured in your thoughts - simply because the eyebrow area is a very individual issue , which requires the most detailed (and deep) study. Fortunately, with something like a browlift, the task becomes much more manageable. Why is this so, says plastic surgeon Alexander Vdovin.
When and why do you need a browlift? After upper blepharoplasty, patients do not always get the result they originally wanted. A brow lift, or brow lift, may be recommended if there is severe ptosis of the upper third of the face, a large number of wrinkles and creases (folds) on the forehead and between the eyebrows, loss of firmness, decreased elasticity of the skin, and lack of sufficient muscle tone in this area. Also, indications for brow lifting are a large number of small wrinkles around the eyes and in the temporal zone, loose skin and sagging facial tissues.
Browlifting helps maintain an open, youthful look, get rid of wrinkles on the forehead and between the eyebrows, and gain an attractive appearance by restoring the elasticity and firmness of the skin in this area. Brow lift is used for patients of all age categories. Browlifting can be used either independently or in combination with other surgical interventions - such as SMAS (non-surgical facial rejuvenation technique) and minimally invasive rejuvenation techniques (
Brow lift with an incision above the eyebrow
A brow lift with an incision above the eyebrow is an outdated technique and is rarely performed due to its high morbidity. The incision is made above the eyebrow and leaves a fairly noticeable scar. Suitable for older patients or patients with a low and wrinkled forehead, in whom such a scar may not be noticeable.
The advantage of a brow lift with an incision above the eyebrow is only one: the operation is performed under local anesthesia.
This technique has a high potential for creating an unnatural, surprised look and does not have the longest lasting effect.
Contraindications to browlifting
Like any surgical intervention, eyebrow plastic surgery has contraindications . These include the following conditions:
- pathologies of the heart and blood vessels;
- disorders of the thyroid gland;
- infectious diseases;
- disruption of internal organs;
- the presence of tumors in the body;
- blood clotting disorder;
- severe skin lesions;
- low elasticity of the epidermis.
If contraindications are ignored, serious complications may develop, so you must make sure that they are absent.
Transpalpebral excision of the muscles of the nose (excision of the muscles of the glabella through the upper eyelid)
Excision of the glabella muscles is carried out through an incision in the upper eyelid, which is used in blepharoplasty. This technique allows you to raise the inner corners of the eyebrows, and also perfectly eliminates the so-called “frowning expression” caused by pronounced wrinkles in the forehead and bridge of the nose. The effect of transpalpebral excision of the muscles of the nose is comparable to Botox injections, but significantly exceeds the long-term results. In combination with lateral eyebrow lifting, the method allows you to get rid of the drooping of the middle part of the eyebrow and wrinkles in the bridge of the nose, which in terms of aesthetic results is not inferior to endoscopic or coronal lifting of the forehead and eyebrows.
Leave a comment →
- Public in
- How it's done
- Message from
- doctorusupov
Rehabilitation
The rehabilitation period after a thread facelift is 2-3 days. After endoscopic surgery – up to 10 days. Particular attention must be paid to caring for puncture sites and skin incisions to prevent infection and related complications.
During the month after the procedures, you will have to observe some restrictions. During this period you cannot:
- actively engage in sports;
- sunbathing;
- visit the sauna, solarium;
- strain your facial muscles too much.
In addition, it is necessary to avoid sudden changes in temperature and increases in blood pressure. Therefore, it is worth temporarily protecting yourself from stress and avoiding long trips.
In the first days after surgery, cold compresses can be used. They will help get rid of swelling faster and prevent the formation of hematomas.
Features of the operation
A forehead and eyebrow lift is performed under general anesthesia and lasts up to 1.5 hours. Most of the body's visible reactions to the intervention (bruises, tissue swelling) disappear without a trace by the end of the third week of rehabilitation. If the operation is performed using minimally invasive endoscopic technology - by the end of the first week.
The result achieved with a facelift lasts for an average of 10 years. Do you want to see what possibilities for rejuvenation and appearance correction this technique provides? With the results of forehead and eyebrow lifting operations performed by K.E. Avdoshenko, can be found in the “Before and After” section on the website.